based on the clinical history and presentation, what disease is this soldier most likely to have?
Definition of Clinical Reasoning:
During clinical encounters with patients, experienced physicians engage in numerous clinical tasks, including listening to the patient'southward story, reviewing the patient's past records, performing a physical examination, choosing the advisable investigations, providing advice or prescribing medications, and/or ordering a consultation. These behaviors which provide the basis of clinical reasoning are influenced and driven by "what" physicians retrieve about and "how" they think.
Clinical Reasoning Principle:
New knowledge is best acquired in the context of application of that knowledge in the cases (case based learning and longitudinal mentorships). Forth with factual information stored in long-term retentiveness, the learner continues to develop retentiveness schemes for representing and relating the clinical problems in reasoning strategies.
Clinical Reasoning:
- Is a procedure by which clinicians collect, process, and interpret patient information to develop an action programme;
- Creates a story from the patient'due south history, physical exam, test results and serial observation;
- Serves to enhance acquisition and storage of cognition through repeated exposure to real case examples;
- Helps the learner develop memory schemes for representing and relating clinical problems.
- Learning for clinical reasoning is driven by repeated exposures to existent instance examples that illustrate multiple aspects of clinical reasoning. Repeated exposures to these cases enhance acquisition and storage of noesis in long-term memory.
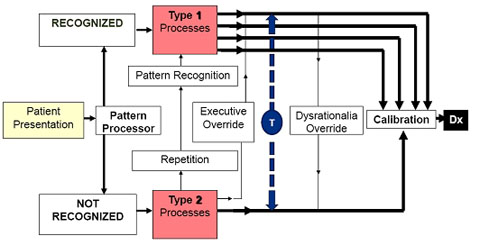
Ii-Procedure Model of Clinical Reasoning
- Type i (Intuitive) processes are very fast – used by experts near of the time
- Type 2 (Rational) processes are slower, deliberate, and more reliable and focus more than on hypothesis and deductive clinical reasoning (Hypothetical- Deductive Reasoning)
- Repetitive operation of Blazon 2 leads to Type 1 (recognition: as you see more cases and use Blazon ii process effectively, you volition build your own illness scripts and your ability to use Blazon i process in medicine volition ameliorate)
- Blazon two processing tin override Type 1 (rational override)
- Type one processing can override Type two (dysrational override)
- The Cognitive Miser Function encourages default to Type 1. Most errors also take identify in Blazon 1 processing.
Overview of the Clinical Reasoning Process
Obtain and filter data.
- Information may exist obtained primarily through reading, visual imagery, and listening.
- Other sensory input (e.g., tactile, olfactory) may be obtained.
Formulate an initial gear up of hypotheses.
- This gear up of hypothesis is formulated in the context of identified questions and issues in the electric current example, as well as a knowledge base of prior cases (using illness scripts and pattern recognition).
- Experts speedily develop a small gear up of hypotheses with minimal clinical data to represent the problem to be solved. Curt-term memory tin can actively handle just most five items at in one case.
- Experts volition mostly have the final diagnosis in this set within 5 minutes of starting. Novice and intermediate learners will have longer to develop a set up of hypotheses.
Obtain additional information as directed by initial hypotheses.
- The initial small set of hypotheses forms a framework for boosted focused information gathering. This process is repeated and refined. Novices and intermediates have more iterations of this process.
Use a reasoning strategy: Hypothetical- Deductive reasoning (deductive v. inductive) to process the information in the clinical context of the instance.
- Hypothetical- Deductive Reasoning: works from general to specific. Develop hypotheses to explain a patient's clinical problem and apply collected data to test the hypotheses in order to effort and confirm or exclude a hypothesis. In a hypothetical-deductive procedure, a classic rank-ordered list of differential diagnoses is generated.
- The process goes: if - then - simply - therefore (yes, no)
- If we take sure information, and then sure hypotheses may be true, but we examination against farther information, and therefore it is true or non.
- This is alike to the scientific principle, in which one tries to prove a hypothesis.
The man torso is very circuitous, and nosotros cannot obtain all information we want, so that regardless of the reasoning process utilized, we can never absolutely bear witness or disprove most hypotheses in many cases. We derive the 'most probable' diagnosis, but we may need to eventually consider others if more information becomes available or the effect is different than expected.
Perform an analysis of hypotheses by probabilistic and crusade-outcome means.
- Hypotheses are refined past cause-result analysis to apply principles of pathophysiology (such equally biomedical cognition and noesis about basic science concepts) and determine if a hypothesis is based upon a sound scientific basis.
- Prove-based medicine is another description of this process. If tests are performed, such every bit laboratory tests, calculated results for test sensitivity, specificity, positive predictive value, and negative predictive value are useful in analysis.
Codify a terminal diagnosis/hypothesis (Based on the above mentioned steps) and test the final diagnosis/hypothesis.
- Test confronting positive and negative findings and standard criteria for description of a disease procedure.
- Working diagnoses for patient are finalized merely later they are assessed for their adequacy in explaining all positive, negative, and normal clinical findings.
- The pathophysiologic reliability of the diagnosis is a check on the reasonableness of causal linkages between clinical events, ascertained from utilize of biomedical knowledge.
- Does the diagnosis fit with cause and outcome? Is the diagnosis consistent with pathophysiologic principles?
Consider other possible diagnoses.
- To diminish the possibility of premature closure, assume your working diagnosis is wrong and then consider alternative diagnoses.
Evaluate the procedure. (Finish, Recall, Human activity, Review): Diagnostic time out
Clinical Reasoning Steps
1. Patient's story:
two. Information conquering:
- Data may exist obtained primarily through reading, visual imagery, and listening.
- Other sensory input (e.g., tactile, olfactory) may exist obtained.
- This includes pertinent positives and negatives from the history, focused physical exam and targeted investigations
3. Authentic problem representation:
- A brief summary where patient specific details are translated into appropriate medical terminology
- Translating the story into abstractions (trouble representation with semantic qualifiers) fosters retrieval of relevant "Illness scripts"
- Semantic qualifiers: paired opposing descriptors that tin can exist used systematically to compare and dissimilarity diagnostic considerations: abrupt/dull, acute/chronic, tender/non-tender, productive/nonproductive, insidious/abrupt, proximal vs. distal. "Semantic qualifiers" serve like Google search terms
- Should include the Cardinal/forceful features(History, physical exam, and tests, pathophysiology, affliction form, memorable cases, recent readings, pearls)
4. Illness scripts:
- A narrative structure for recalling the key attributes of a typical example presentation of a status or a diagnosis
- Employ typical cases to build prototypes
- Include risk factors, fundamental/forceful features
- Build cognition stores retrieved past clinical presentations
- For example, the illness script for pneumonia differs from that for congestive heart failure in the constellation of features. You will learn features mutual to both AND which features favor one condition over some other.
5. Hypothesis generation, prioritization and evaluation:
- Hypothesis is generated early on in the encounter.
- They are based on cues acquired from the patient past observation and attentive listening.
- Hypothesis must not exist generated too early, that is, before the patient provides suggestive and useful cues.
- More than ane hypothesis is almost ever needed, as the best evaluation of a hypothesis is past comparison with alternatives.
Hypothesis Generation:
1. Hypothetical- Deductive Reasoning:
- Develop hypotheses to explain a patient'southward clinical problem and apply nerveless data to exam the hypotheses in order to endeavour and confirm or exclude a hypothesis.
- In a hypothetical-deductive procedure, a classic rank-ordered list of differential diagnoses is generated.
- The process goes: if - then - but - therefore (yes, no)
- If nosotros have certain data, and so sure hypotheses may exist true, but we test against farther information, and therefore it is true or not.
- This is akin to the scientific principle, in which i tries to testify a hypothesis.
ii. Compare and Dissimilarity (Pattern recognition) ( as yous advance from novice to skilful you will be using this type of reasoning more often)
- Blueprint recognition: matching the patients problem representation to an appropriate disease script
- Verify, reject and refine hypothesis past additional ascertainment, exam, test etc
Prioritize the Hypothesis or Differential: Based on the most likely hypothesis prioritize your differential diagnosis:
1. Compare and contrast two plausible hypotheses and prioritize among the competing options.
2. Compare/contrast unlike illness scripts with the patient'due south problem representation looking for best match
Exam the final diagnosis/hypothesis (Hypothesis Evaluation): Perform an analysis of hypotheses by probabilistic and crusade-effect means. Hypotheses are refined by cause-effect assay to utilize principles of pathophysiology (such as biomedical knowledge and knowledge about basic science concepts) and decide if a hypothesis is based upon a sound scientific basis.
- Test against positive and negative findings and standard criteria for description of a disease process.
- Working diagnoses for patient are finalized merely later they are assessed for their adequacy in explaining all positive, negative, and normal clinical findings.
- The pathophysiologic reliability of the diagnosis is a check on the reasonableness of causal linkages betwixt clinical events, ascertained from apply of biomedical knowledge. Does the diagnosis fit with cause and consequence? Is the diagnosis consequent with pathophysiologic principles?
Synopsis: The above detailed steps may not be immediately recognizable or flow in the same sequence in the context of bodily clinical reasoning. Experts utilise blueprint recognition with non-analytic cognitive processing during the initial phases of considering a novel clinical example, and then employ analytic processing in hypothesis testing. Novices may work the other style round. However, these two forms of reasoning can be interactive and not sequential. They are complementary contributors to the overall accurateness of the clinical reasoning process, each one influencing the other. Persons who use both perform better than persons using either not-analytic or analytic approaches alone.
Glossary
| Key facts | Forceful features |
| Abstracting terms | Semantic qualifiers |
| Example formulation | Problem representation |
| Typical presentation | Illness script |
hazelwoodexambeir1955.blogspot.com
Source: https://medicine.uiowa.edu/internalmedicine/education/master-clinician-program/students/clinical-and-diagnostic-reasoning
0 Response to "based on the clinical history and presentation, what disease is this soldier most likely to have?"
Post a Comment